Prostate Cancer Is on the Rise. A Faster MRI Could Help More Men Get Answers.

If prostate cancer feels like it is in the news more often lately, that impression is not far off. It is now the most commonly diagnosed cancer in the United States. For 2026, the American Cancer Society projects about 333,830 new cases, placing it roughly on par with breast cancer and, by most recent estimates, narrowly ahead of it as the single most common cancer diagnosis. Incidence has been climbing by close to 3% a year since 2014.
There is an important nuance behind that rise. Much of the recent increase has come from cancers found at a more advanced stage, when they are harder to treat. That is part of why how and when prostate cancer is found has drawn so much attention. Finding clinically significant prostate cancer, meaning the kind more likely to grow or spread, while it is still confined to the prostate gives men and their doctors the widest range of options.
This is the backdrop for one of the more practical shifts in prostatecare: MRI has become central to evaluation, and the scan itself is gettingfaster and more widely available. Understanding what that means can help youmake sense of your own pathway and have a clearer conversation with your careteam.
A growing problem worth paying attention to
Beyond the headline numbers, prostate cancer accounts for nearly one third of cancer diagnoses in men and remains the second-leading cause of cancer death in men, behind lung cancer. The burden is not limited to the United States. In the United Kingdom, there are roughly 56,000 diagnoses and 12,000 deaths each year, making it the most common cancer in men there as well.
None of this means that every man needs to act in the same way, or thatmore testing is automatically better. Whether and when to be screened forprostate cancer is a shared decision that depends on your age, risk factors,and preferences, and guidance varies by region. In the United States, theUSPSTF frames PSA screening for men aged 55 to 69 as an individual decision tomake with a clinician. In Europe, the EAU supports a risk-adapted approach. Thepoint is not that everyone should be scanned, but that when a man does needimaging, getting an accurate scan quickly matters.
For decades, evaluation leaned heavily on the PSA blood test followed by a systematic biopsy, an approach that could miss significant cancers while also finding many that would never cause harm. The arrival of prostate MRI over the past decade is widely regarded as the biggest change in how the disease is evaluated in a generation.
MRI uses a strong magnet and radio waves, with no radiation, to produce detailed images of the prostate. Its value is twofold. When MRI shows a suspicious area, it allows a targeted biopsy aimed at that specific spot, which improves the detection of clinically significant cancer. And when MRI looks reassuring, it can help some men avoid an immediate biopsy altogether. It is worth being precise here: MRI helps decide where and whether to biopsy, but it does not diagnose cancer on its own. A diagnosis still depends on tissue examined by a pathologist, and a reassuring MRI lowers the chance of significant cancer without reducing it to zero.
Guidelines in the United States, Europe, and the UK now recommend MRI before biopsy for men with suspected prostate cancer. The UK moved early and decisively: NICE guidance embedded multiparametric MRI into the standard diagnostic pathway, so that men are typically scanned before any decision about biopsy. That has made MRI-before-biopsy routine across the National Health Service.
Access is still uneven, which is exactly why the technology matters. Estimates suggest about 35% of US prostate cancer patients received an MRI in 2022, and that around 62% of men in England and Wales who needed a prostate MRI received one in 2019. Worldwide, researchers estimate roughly four million prostate MRIs are needed each year, and demand is expected to rise as cases climb. When a scan is faster and cheaper, more of the men who need imaging can actually get it without longer waits. The UK is also running TRANSFORM, a major trial examining how best to screen for prostate cancer, with MRI as a central part of the design.
A prostate MRI is built from several imaging sequences, which are different ways of picturing the same tissue. A multiparametric MRI (mpMRI) typically uses three: T2-weighted imaging (T2W) for anatomy, diffusion-weighted imaging (DWI) with its ADC map for how densely tissue is packed, and a dynamic contrast-enhanced (DCE) sequence, which requires a gadolinium dye injected through an IV.
A biparametric MRI (bpMRI) keeps the first two and drops the contrast step. That single change is what makes it faster and simpler.
The obvious question is whether dropping a step means missing cancers. The largest study to test this head to head is the PRIME trial, published in JAMA in September 2025. Across 22 hospitals in 12 countries, men were scanned both ways so the two could be compared in the same person. The biparametric scan found clinically significant prostate cancer in about 29% of men, essentially identical to the multiparametric scan, with only a fraction of a percent between them.
The investigators added one important condition. The benefit holds when image quality is high, using modern scanners; where quality is lower, the contrast sequence may still add useful information. So bpMRI is a strong option for many men rather than the automatic choice everywhere, and the field continues to study it. For patients, the practical payoff is real: a shorter time in the scanner, no IV or contrast dye, and broader availability at lower cost.
Reading prostate MRI well takes experience, and results can vary from one radiologist to another. This is where artificial intelligence is being studied as a support tool, helping flag suspicious areas, measure the prostate, and bring more consistency to how scans are scored.
The evidence is encouraging and still developing. In the international PI-CAI study, an AI system reached higher overall accuracy than a pool of 62 radiologists reading under study conditions (an AUROC of about 0.91 versus 0.86). In a separate reader study, radiologists who used AI assistance performed better than those who did not, and the gains were largest for less-experienced readers. Several studies have also found that AI assistance can reduce differences between readers and shorten reading time.
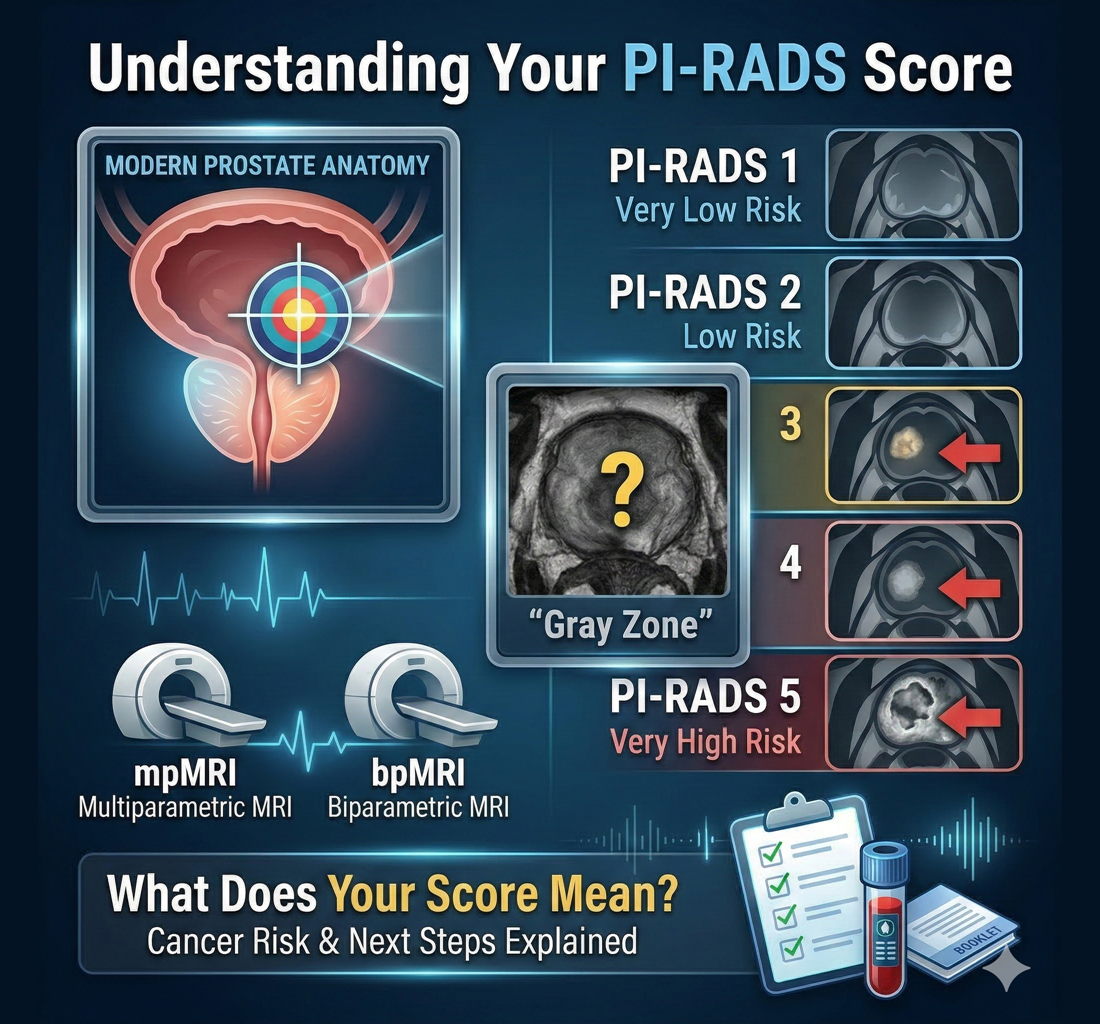
MRI has genuinely improved prostate cancer evaluation, but it has limits worth knowing. It can miss some clinically significant cancers, its accuracy depends on scan quality and reader experience, and a reassuring result lowers risk without eliminating it. A suspicion score such as PI-RADS in the US and much of Europe, or the Likert scale used under NICE guidance in the UK, describes how suspicious an area looks. It is not a diagnosis.
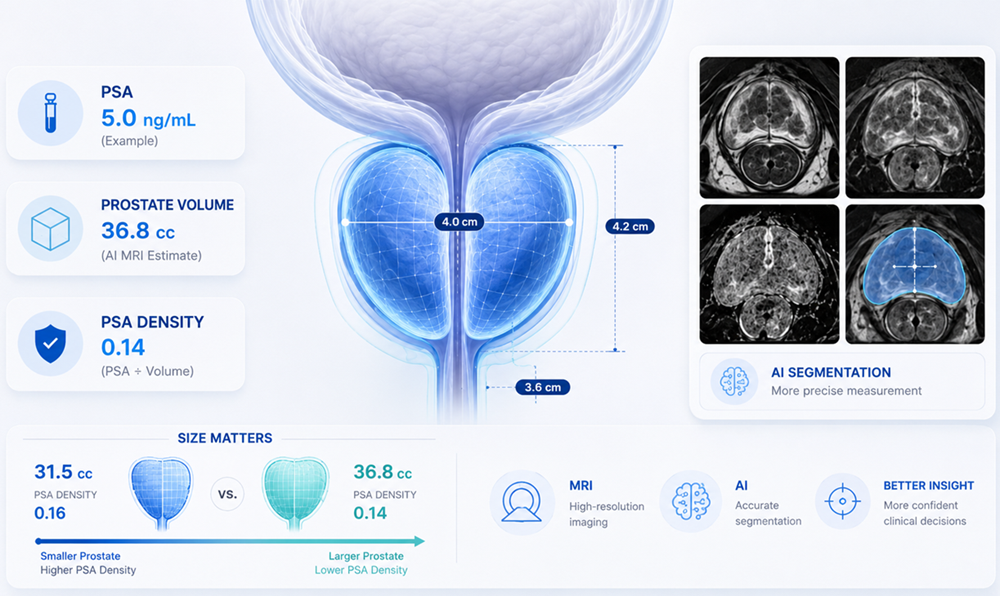
That is why decisions rarely rest on imaging alone. Physicians usually weigh the whole picture: your PSA level and trend, PSA density (your PSA relative to prostate size), prostate volume, the MRI findings and score, where any suspicious area sits, your age, family history, ancestry where clinically relevant, prior biopsy results, symptoms, and your own preferences. Two men with similar numbers can still receive different recommendations once everything is considered.
For more information about PI-RADS see: Understanding Your PI-RADS Score
If you already have a prostate MRI, you may want an additional perspective on it. DeepView Imaging, a service of Precision Prostate Consulting, provides an AI-supported second analysis of a prostate MRI using ProstatID, software that is FDA-cleared, CE-Marked, and UKCA-Certified for prostate MRI analysis. You can securely upload an existing scan and receive a report with color overlays that mark regions the software flags as suspicious, drawn from a model trained on biopsy-confirmed cases. Because ProstatID works from the biparametric data (T2W, DWI, and the ADC map) and does not use the contrast sequence, it is compatible with both bpMRI and mpMRI scans. The goal is to give you and your care team another perspective on information already contained within your MRI. It does not replace your radiologist, urologist, or treating physician, and you can share the results with your doctor when discussing next steps.
Prostate cancer is becoming more common, and the tools to find significant disease earlier and more accurately are getting better at the same time. Faster, contrast-free MRI can widen access without sacrificing accuracy when image quality is high, and AI is emerging as a useful aid for the radiologists who read these scans. For you, the practical takeaway is encouraging: a clearer, quicker path to answers is increasingly within reach. The scan is still one piece of a larger picture, a suspicion score is not a diagnosis, and a biopsy remains the usual route to certainty, so the most valuable step you can take is to understand what your scan shows and bring your questions to the physician guiding your care.
- Siegel RL, Kratzer TB, Wagle NS, Sung H, Jemal A."Cancer statistics, 2026." CA: A Cancer Journal for Clinicians. 2026.doi:10.3322/caac.70043
- American Cancer Society. Cancer Facts & Figures2026. Atlanta: American Cancer Society; 2026. (Also: NCI SEER Cancer StatFacts, Common Cancer Sites.)
- Ng AB, Asif A, Agarwal R, et al. "Biparametric vsMultiparametric MRI for Prostate Cancer Diagnosis: The PRIME DiagnosticClinical Trial." JAMA. 2025;334(13):1170–1179. doi:10.1001/jama.2025.13722
- University College London. "Millions of men couldbenefit from faster scan to diagnose prostate cancer." September 2025.ucl.ac.uk/news
- Saha A, Bosma JS, Twilt JJ, et al. "Artificialintelligence and radiologists in prostate cancer detection on MRI (PI-CAI): aninternational, paired, non-inferiority, confirmatory study." LancetOncology. 2024;25(7):879–887.
- National Institute for Health and Care Excellence(NICE). "Prostate cancer: diagnosis and management" (NG131).nice.org.uk/guidance/ng131
- U.S. Preventive Services Task Force. "ProstateCancer: Screening." uspreventiveservicestaskforce.org
- American College of Radiology. PI-RADS (ProstateImaging Reporting and Data System). acr.org
- Bot Image, Inc. ProstatID regulatory announcements: FDAclearance; CE Mark (October 2025); UKCA certification (November 2025).botimageai.com