Understanding Prostate Biopsy Decisions: What Patients Should Know

Hearing that you may need a prostate biopsy can feel overwhelming. For many patients, it is the first time they have had to think seriously about prostate cancer, MRI scans, PSA levels, or what happens next.
One of the most important things to understand is that a recommendation for further testing or even a possible biopsy does not automatically mean you have prostate cancer.
In recent years, prostate cancer evaluation has become much more advanced and personalized. Today, doctors often use several pieces of information together, including PSA levels, MRI findings, personal risk factors, and increasingly, AI-supported imaging analysis tools, to better understand what may actually be happening inside the prostate.
The goal is not simply to perform more biopsies.
The goal is to make the most informed decision possible for each patient while reducing unnecessary procedures whenever safely possible.
Why Prostate Cancer Decisions Can Feel So Uncertain
One reason prostate cancer evaluation can feel difficult to navigate is that several things can be true at the same time.
MRI is extremely valuable. Biopsy is still the only definitive way to confirm cancer. Some prostate cancers are aggressive and require treatment, while others grow slowly and may never become life-threatening.
For patients, that can create a lot of emotional uncertainty.
You may hear:
- “Your PSA is elevated.”
- “Your MRI showed something suspicious.”
- “We should monitor this.”
- “We may need a biopsy.”
- “This may not be serious.”
That can feel overwhelming, especially when you are trying to understand what happens next and whether immediate treatment is truly necessary.
What doctors are ultimately trying to determine is not simply whether cancer exists, but whether there is evidence of a more aggressive cancer that is likely to grow, spread, or require treatment.
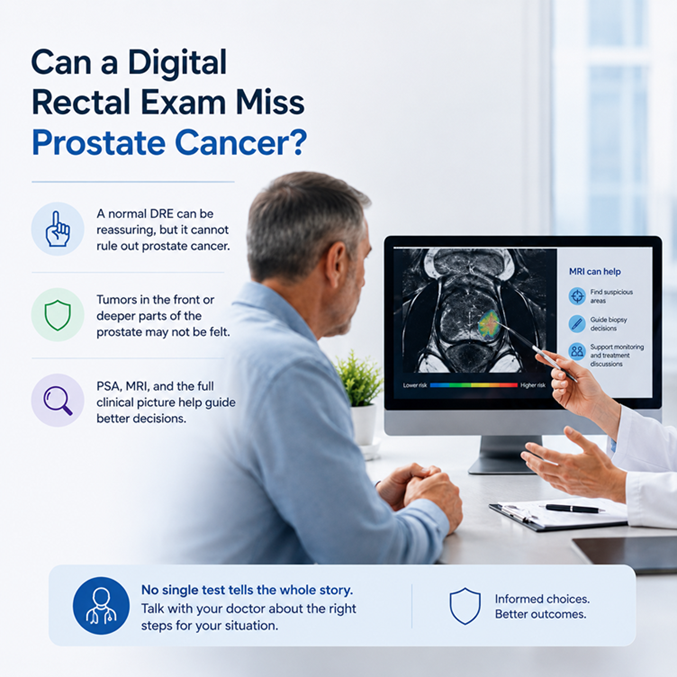
For many patients, the process begins with a PSA blood test.
PSA, or prostate-specific antigen, is a protein produced by the prostate gland. Higher PSA levels can sometimes be associated with prostate cancer, but PSA can also rise for several non-cancerous reasons, including aging, benign prostate enlargement, inflammation, or infection.
That is why most doctors do not make biopsy decisions based on PSA alone.
Instead, doctors look at PSA as one part of a much larger picture. They may also consider MRI findings, PSA density, family history, age, prior biopsy history, and other clinical risk factors before deciding whether a biopsy is truly necessary.
Modern prostate cancer evaluation is much more individualized than it was years ago, which is one reason two patients with similar PSA levels may receive very different recommendations.
Over the past decade, prostate MRI has become a central part of how doctors evaluate many men with an elevated PSA or other signs that prostate cancer might be present. Instead of going straight to biopsy in every case, doctors now often use MRI first to look for areas that appear more or less suspicious. This has made the pathway more accurate and more individualized.
Many centers now perform either multiparametric MRI (mpMRI) or biparametric MRI (bpMRI). A bpMRI is a contrast-free exam that usually includes high-quality T2-weighted and diffusion-weighted imaging. An mpMRI adds a third sequence called dynamic contrast-enhanced imaging, which uses IV contrast dye. In many men having a first evaluation before biopsy, a high-quality bpMRI can detect clinically significant prostate cancer about as well as mpMRI when the scan quality is high and the images are read by experienced prostate radiologists or well trained AI system.
MRI does not diagnose cancer by itself, but it helps doctors decide what to do next. If MRI shows a clearly suspicious area, that area can be sampled with a targeted biopsy, sometimes along with additional sampling depending on the patient’s risk factors, prior biopsy history, age, and local practice. If MRI is negative or low risk, some men may be able to avoid an immediate biopsy, but only when the rest of the clinical picture is reassuring. Doctors still look at factors such as PSA density, family history, prior biopsy results, and how strong the overall suspicion remains. A negative MRI lowers risk, but it does not reduce the chance of significant cancer to zero.
MRI reports are usually summarized with a risk score. Many practices use PI-RADS, while some systems, including NICE guidance in the UK, use a 5-point Likert scale. These scores estimate how suspicious a finding looks, but they are not the same as a cancer diagnosis. MRI also has limitations: some significant cancers may still be missed, and scan quality and reader experience matter a great deal. That is why MRI works best when it is combined with good clinical judgment rather than used alone.
Although bpMRI is increasingly supported for many first-diagnostic situations, mpMRI still has an important role. Doctors may prefer mpMRI when image quality is suboptimal, when suspicion remains high after a prior negative biopsy or a prior negative bpMRI, when the patient is being followed on active surveillance, when previous prostate treatment may have changed the gland, or when evaluating for recurrence after treatment. In other words, bpMRI is often enough for the right patient in the right setting, but mpMRI is still preferred in some higher-uncertainty situations.
One of the most surprising things many patients learn is that not all prostate cancers behave the same way.
Some prostate cancers are aggressive and require treatment. Others grow so slowly that they may never cause symptoms or shorten a person’s life expectancy.
Because of this, some patients diagnosed with lower-risk prostate cancer may be candidates for active surveillance instead of immediate surgery or radiation therapy.
For patients on active surveillance, monitoring usually continues through regular PSA testing, repeat MRI imaging, follow-up evaluations, and sometimes periodic biopsies when appropriate.
The goal is not to ignore the cancer.
The goal is to watch it carefully while avoiding unnecessary treatment unless there are signs the disease is becoming more aggressive.
For many patients, this approach can help preserve quality of life while still maintaining close medical monitoring.
Reading prostate MRI is highly specialized.
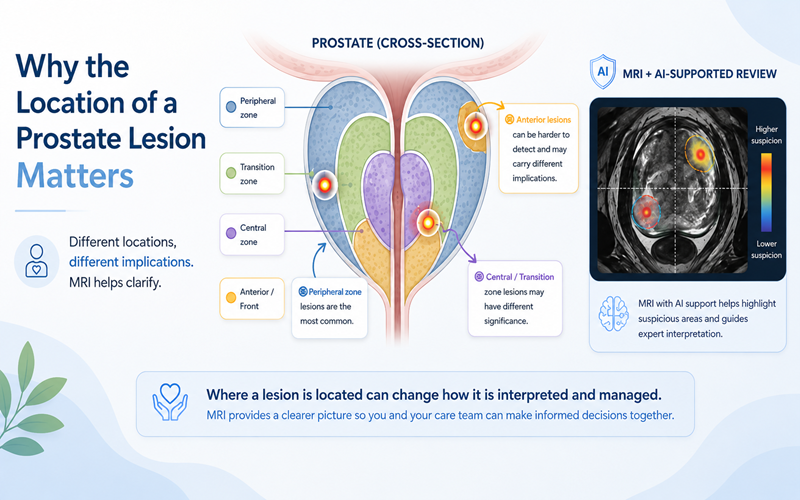
Even among experienced physicians, subtle prostate MRI findings can sometimes be interpreted differently. Factors such as image quality, lesion location, and reader experience can all influence interpretation.
Because prostate MRI interpretation can be complex, many hospitals and imaging centers place significant emphasis on experienced radiologists, standardized reporting systems, multidisciplinary review, and high-quality imaging protocols.
Patients are often surprised to learn how much expertise and collaboration may go into interpreting a single prostate MRI accurately.
This growing focus on imaging quality and consistency is also one reason AI-supported imaging analysis is receiving increasing attention in prostate cancer care.
As prostate MRI becomes increasingly important in clinical decision-making, some physicians and imaging centers are beginning to use AI-supported imaging analysis as an additional layer of review.
These systems are designed to assist radiologists by analyzing MRI patterns using technology trained on large datasets linked to biopsy-confirmed results. Researchers are studying whether AI may help improve consistency, identify suspicious regions, and support clinical interpretation in difficult or subtle cases.
Importantly, AI is not intended to replace physicians.
Instead, these tools are being explored as a way to support doctors as they evaluate MRI findings alongside laboratory data, clinical history, and patient risk factors.
For patients, the potential value of these tools may ultimately come down to something very simple:
Helping reduce uncertainty and supporting more informed decision-making.
Today, doctors have more tools than ever before to evaluate prostate cancer risk, including PSA testing, MRI imaging, targeted biopsy techniques, and emerging AI-supported imaging analysis.
But the most important part of the process is still thoughtful decision-making between patients and their care teams.
The goal is not simply to find cancer.
The goal is to better understand risk, avoid unnecessary procedures when safely possible, identify higher-risk disease accurately, and help patients move forward with greater clarity and confidence.
Sources:
Clinical Guidelines & Medical Organizations
- National Comprehensive Cancer Network (NCCN) Prostate Cancer Early Detection Guidelines
NCCN Guidelines for Prostate Cancer Early Detection - American Urological Association (AUA) guidance on prostate MRI and biopsy
American Urological Association - European Association of Urology (EAU) Prostate Cancer Guidelines
EAU Prostate Cancer Guidelines
MRI & Prostate Cancer Research
- JAMA Oncology research on MRI and clinically significant prostate cancer detection
JAMA Oncology - PROMIS Trial: MRI compared with biopsy pathways in prostate cancer detection
The Lancet PROMIS Trial - PI-RADS prostate MRI reporting system
American College of Radiology PI-RADS Information
Active Surveillance & Risk Stratification
- Active surveillance in prostate cancer management
UroToday Active Surveillance Overview - National Cancer Institute overview of prostate cancer treatment and surveillance
National Cancer Institute Prostate Cancer Information