Why Lesion Location Matters
When most patients receive the results of a prostate MRI, their attention naturally goes to the findings section. They look for words like lesion, suspicious, PI-RADS, or cancer.
What often receives far less attention is where the lesion is located. Yet location is one of the first things physicians and radiologists consider when reviewing a prostate MRI.
The reason is simple. The prostate is not one uniform organ. It contains several distinct regions, each with its own anatomy, its own typical appearance on imaging, and its own implications for cancer detection. Knowing where a lesion sits can matter nearly as much as knowing that it is there.
A quick note on terms before we begin. A lesion is simply an area that looks different from the surrounding tissue and may deserve a closer look. Clinically significant prostate cancer refers to cancer that is more likely to grow or spread and cause harm, as opposed to slow-growing (indolent) disease that may never cause problems. Physicians often gauge significance using the Gleason score or Grade Group after a biopsy.
The prostate has its own internal geography
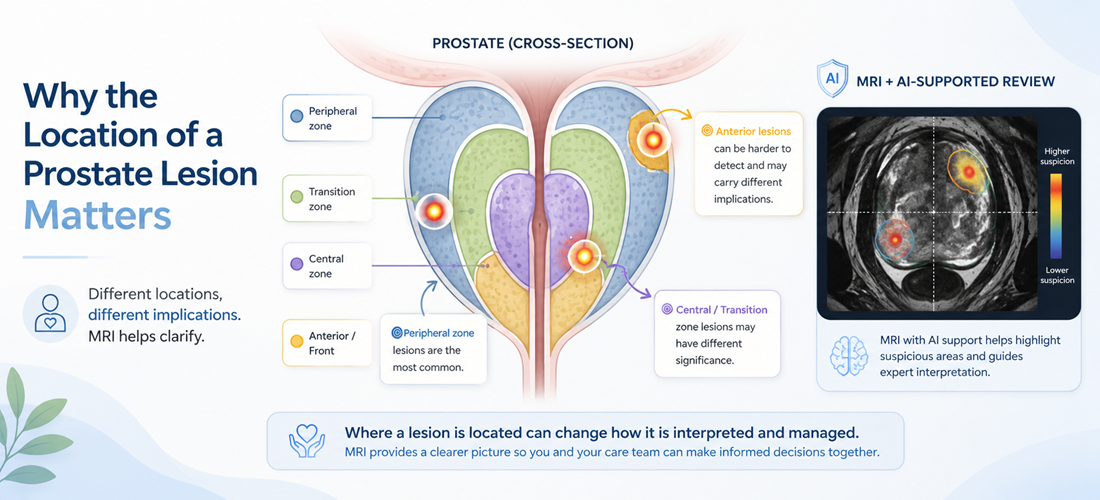
Many patients are surprised to learn that the prostate has an internal map. Rather than being made of one kind of tissue, the gland contains several anatomical zones, and each looks and behaves differently on MRI.
Understanding these zones helps explain why some lesions are easier to recognize, why others are harder to interpret, and why radiologists pay such close attention to location. It also helps explain why two findings that sound similar on paper can be evaluated quite differently.
The peripheral zone is typically the largest region of the prostate, especially before age-related transition-zone enlargement becomes prominent, and wraps around much of the outer and back portion of the gland. It is also where the majority of clinically significant prostate cancers are found. In many studies, a large share of significant cancers, often cited as roughly 70 to 75 percent, arise here, which is one reason radiologists spend considerable time on this area.
The peripheral zone usually has a fairly uniform appearance on MRI. When tissue that normally looks consistent develops an abnormal area, that change can stand out more clearly. That relative uniformity is part of what makes the peripheral zone a productive place to look.
Even so, not every cancer starts here, and a normal-looking peripheral zone does not settle the question on its own.
The transition zone sits deeper in the gland and surrounds the urethra, the tube that carries urine out of the body. As men age, this region often enlarges because of benign prostatic hyperplasia (BPH), a common and non-cancerous growth of the prostate that affects a large share of older men.
This creates a genuine interpretation challenge. The transition zone can already contain nodules and irregular-looking areas that are entirely benign. Telling ordinary age-related change apart from a suspicious finding can be harder here than in the peripheral zone.
For patients, this means a lesion in the transition zone may be assessed differently, and physicians may weigh additional information before deciding what, if anything, it warrants.
Two remaining regions arise less often but are still part of every complete review. The first is the central zone, which occupies a smaller portion of the prostate and surrounds the ejaculatory ducts. Compared with the peripheral and transition zones, cancers develop here less frequently, but its position and appearance on imaging can still call for careful interpretation. Radiologists review every region of the gland, because clinically significant findings can occasionally turn up in less expected places.
The second is the front of the gland. Toward the front lies the anterior fibromuscular stroma, a band of mostly fibrous and muscular tissue. Cancer rarely originates in this band itself, since it contains little of the glandular tissue where prostate cancer typically begins. But tumors can develop in the adjacent tissue toward the front of the prostate, in the anterior part of the transition zone or the front edge of the peripheral zone.
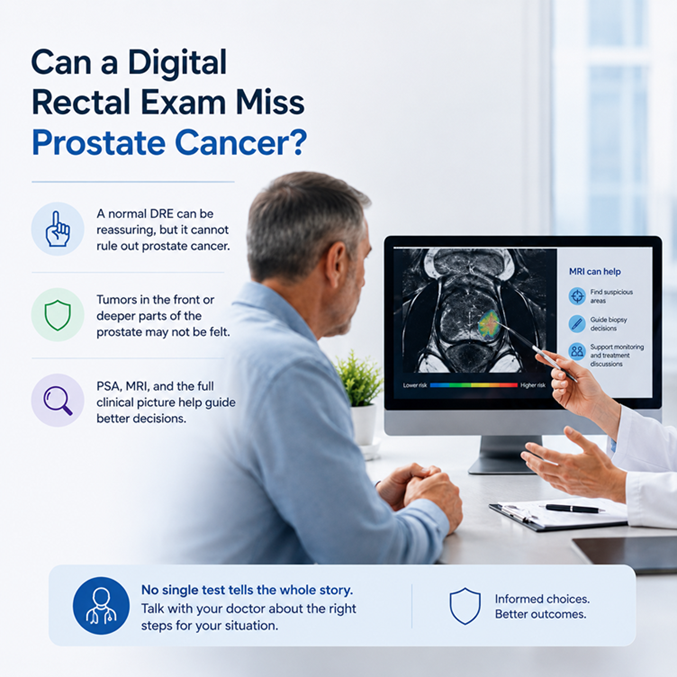
Historically, tumors in this forward region were among the harder ones to detect. A digital rectal examination (DRE), in which a physician feels the prostate through the rectal wall, mainly reaches the back of the gland, so a lesion near the front can be less accessible to touch. MRI changed that. It lets physicians view the front of the prostate directly, helping reveal areas that older methods could miss, which is one reason imaging has become so central to the modern prostate pathway.
Related article: Can a Digital Rectal Exam Miss Cancer?
Radiologists often summarize how suspicious an area looks using a structured score. In the United States and much of Europe, that system is PI-RADS (Prostate Imaging Reporting and Data System), which runs from 1 (very low suspicion) to 5 (very high suspicion). In the United Kingdom, NICE guidance also supports a 5-point Likert scale, which serves a similar purpose. A score describes how suspicious an area appears on MRI. It is not the same as a diagnosis.
Here is where zones matter directly. PI-RADS leans on different MRI sequences depending on location. In the peripheral zone, the diffusion-weighted images (DWI, along with the linked ADC map, which reflect how water moves through tissue) usually carry the most weight. In the transition zone, the T2-weighted images (T2W, which show anatomy and structure) usually lead. So the same-looking spot can be scored differently depending on the zone it occupies, because the radiologist is emphasizing different evidence.
This is also why scan quality and reader experience matter. MRI interpretation can vary, because scan quality, lesion location, reader experience, and the broader clinical context all play a part.
For more information about PI-RADS see: Understanding Your PI-RADS Score
Location rarely stands alone. Physicians usually weigh it alongside many other factors: the PSA level and how it has trended over time, PSA density (the PSA relative to prostate volume), prostate size, the MRI findings and their PI-RADS or Likert score, family history, age, ancestry where clinically relevant, symptoms, other health conditions, any prior biopsy results, and personal preferences.
This is why similar numbers can mean different things in different men. A given finding in a small prostate with a rising PSA may prompt a different conversation than the same finding in a larger gland with stable numbers. Biopsy decisions often depend on the full clinical picture, and guidance frames those decisions as a shared discussion between patient and physician. In the U.S., the AUA and NCCN outline the diagnostic pathway; in Europe, the EAU offers risk-adapted guidance; in the UK, NICE does the same. Screening and biopsy are decisions to weigh with your care team, not steps to assume.
It is also worth remembering that not every prostate cancer needs aggressive treatment. Many low-risk cancers are safely followed through active surveillance, a plan of regular monitoring rather than immediate treatment.
MRI helps identify suspicious areas, guide targeted biopsy, support monitoring, and add anatomical context. What it does not do is diagnose cancer by itself. Diagnosis still depends on a biopsy and the pathology that follows. A negative MRI lowers risk, but it does not reduce that risk to zero.
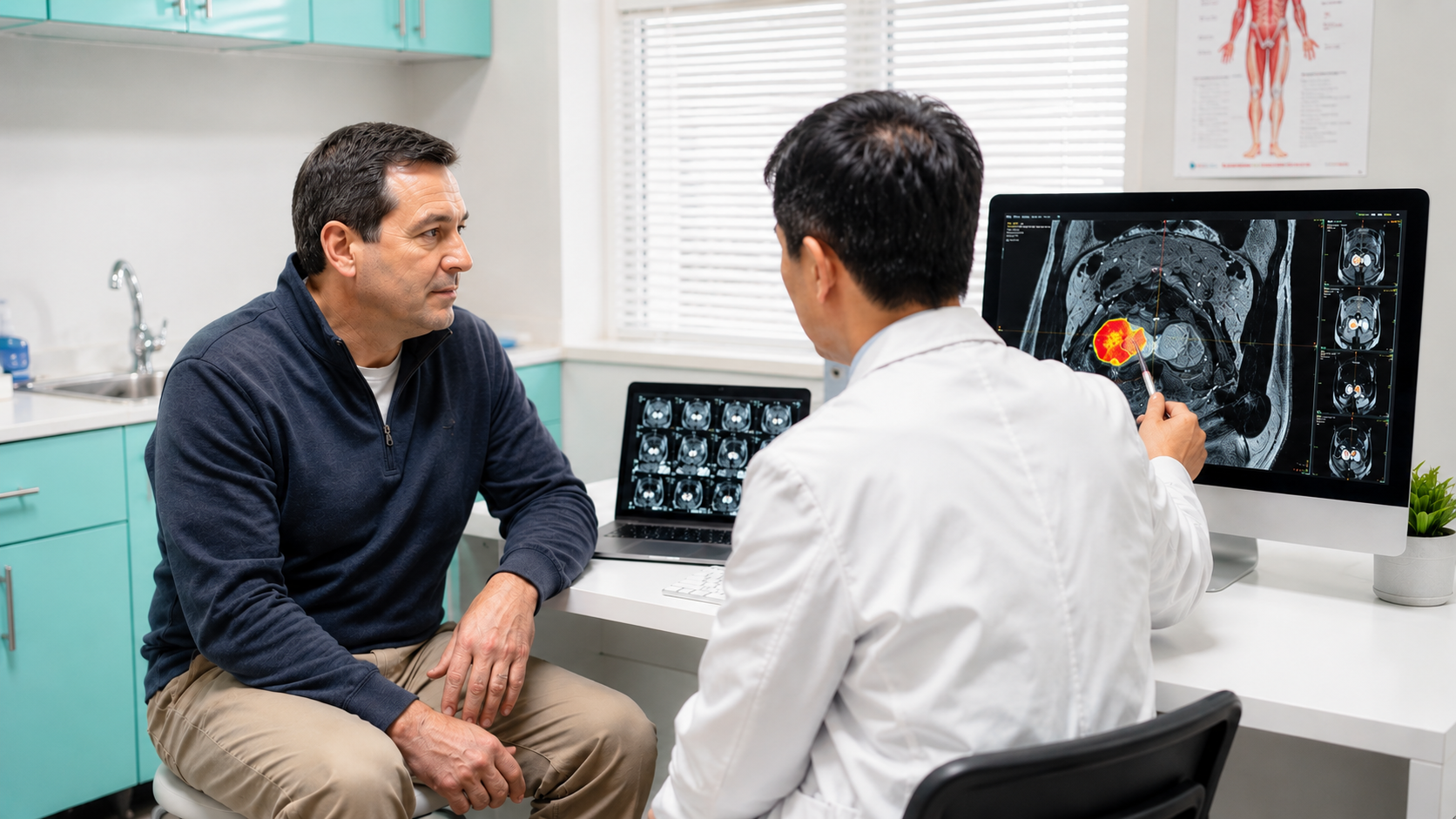
Because location and appearance both matter, some patients choose to obtain a second review of their MRI. Artificial intelligence is increasingly used to assist here. Rather than focusing on a single image, AI can work across the full imaging dataset, measure the prostate and its structures, and highlight regions that may deserve closer attention, including where those regions sit within the gland. AI-supported analysis may help flag areas worth a second look, though physician judgment remains central.
DeepView Imaging provides an AI-supported second analysis of a prostate MRI, powered by ProstatID, an AI software platform that is FDA-cleared in the United States and also CE-Marked (EU) and UKCA-Certified (UK). A patient who already has a prostate MRI can securely upload it and receive a report with color overlays that show the prostate's anatomy and mark regions the software identifies as potentially suspicious, along with where those regions fall within the gland. It analyzes the standard bpMRI sequences (T2W, DWI, and ADC) and does not rely on contrast, so it is compatible with both bpMRI and mpMRI scans. The purpose is to give patients and their care team another perspective on information already contained within the MRI, which they can review together with their physician. DeepView Imaging does not replace a radiologist, urologist, or treating physician, and it does not diagnose cancer.
Where a lesion sits inside the prostate influences how it looks on MRI, how it is scored, and how physicians think about what comes next. Understanding the gland's zones will not tell you what your own scan means, but it can help you ask sharper questions and follow the conversation more closely. The clearest picture comes from putting location together with your PSA, your history, and your physician's judgment, so that decisions about biopsy, surveillance, or treatment rest on the full picture rather than any single detail.
Questions you may want to ask about lesion location:
- Which zone is the lesion in: peripheral, transition, central, or anterior?
- Is it near the apex, base, capsule, urethra, or seminal vesicles?
- Which MRI sequence contributed most to the score?
- What is my prostate volume and PSA density?
- If biopsy is being discussed, how would the lesion's location affect targeting?
Disclaimer: This article is for educational purposes only and is not medical advice. Decisions about screening, biopsy, diagnosis, monitoring, or treatment should be made with your treating physician.
Sources:
- American College of Radiology, ESUR, and AdMeTech Foundation. PI-RADS: Prostate Imaging Reporting and Data System, Version 2.1.
- Weinreb JC, et al. PI-RADS Prostate Imaging Reporting and Data System. European Urology, 2016.
- National Institute for Health and Care Excellence (NICE). Prostate cancer: diagnosis and management (NG131).
- European Association of Urology (EAU). Guidelines on Prostate Cancer.
- American Urological Association (AUA) / SUO and NCCN. Prostate cancer early detection and clinical guidelines.
- McNeal JE. The zonal anatomy of the prostate. The Prostate, 1981.
- Ahmed HU, et al. Diagnostic accuracy of multi-parametric MRI (PROMIS). The Lancet, 2017.
- Kasivisvanathan V, et al. MRI-targeted or standard biopsy (PRECISION). New England Journal of Medicine, 2018.
- U.S. Food and Drug Administration. 510(k) Premarket Notification K212783, ProstatID, decision date July 8, 2022.